
Mike Sutton looks at the journey the diabetes treatment took from the Toronto miracle to mass-production – via a controversial trip to Stockholm
While John Macleod’s colleagues and students at the University of Toronto in Canada were planning their 1921 summer vacations, he was arranging to allocate some of his laboratory space to a freelance researcher. Although Frederick Banting’s project looked very speculative, Macleod offered him this opportunity and assigned a research student, Charles Best, to help him. Macleod then departed for Scotland, unaware that within three years he and Banting – but not Best – would share a Nobel prize.
On returning to Canada in the autumn, Macleod realised Banting and Best were close to a breakthrough in treating diabetes – a condition studied for centuries, yet still incurable. Recognising the project’s importance, Macleod boosted it, and encouraged James Collip – a biochemist on research leave from the University of Alberta – to participate.
After further laboratory work and some clinical trials, they announced the discovery of an effective remedy for diabetes. Within months a major drug company was mass-producing it, even though chemists needed many more years to unravel its molecular structure, and then to synthesise it.
Unfortunately, Macleod, Banting, Best and Collip became embroiled in angry disagreements – some stopping only just short of physical violence – and they left conflicting accounts of how the discovery was made. Untangling this story presented historians with a major challenge, and lessons may still be learned from it.
Origin story
Frederick Banting began studying medicine at the University of Toronto in 1912. After war was declared in 1914 his course was compressed, and in 1916 he became an army medical officer. He was wounded while serving on the western front, and returned home in 1919 with a Military Cross, a fiery temper and a tendency to seek solace in alcohol when under stress.
Despite Banting’s lack of research experience – and limited knowledge of chemistry – he hoped to solve this puzzle
In July 1920 Banting established a practice in London, Ontario, but attracted few patients. Financial insecurity compelled him to postpone marrying his fiancée, Edith Roach, and to undertake part-time teaching at the University of Western Ontario. While preparing a talk on carbohydrate metabolism, he noticed a recent article about diabetes research.
Diabetes was known to result from malfunction of an abdominal organ – the pancreas; autopsies of human patients revealed pancreatic degeneration, and diabetic symptoms appeared in animals whose pancreases were removed. Since a key indicator of diabetes is excess sugar in the urine, doctors assumed the pancreas produced some agent needed for carbohydrate metabolism. If this agent could be isolated, then animal pancreas extracts might benefit human patients with diabetes.
Several researchers pursued this idea, but animal trials were not successful enough to justify tests on human patients. The Romanian Nicolae Paulescu got closest, though the coming of war in 1914 stalled his work. Despite Banting’s lack of research experience – and limited knowledge of chemistry – he hoped to solve this puzzle. But first, he needed a laboratory.
Hard work in the lab
In November 1920 Banting sought an interview with Macleod – a specialist in carbohydrate metabolism – who later recalled: ‘I found that Dr Banting had only a superficial textbook knowledge of the work that had been done… and he had very little practical familiarity with the methods by which such a problem could be investigated in the laboratory.’ Nevertheless, he offered Banting a chance to test his idea.
After some hesitation, Banting abandoned his struggling practice and moved to Toronto – meanwhile, Edith broke off their engagement. Throughout the summer of 1921 he worked with ferocious intensity, undaunted by numerous setbacks which were probably due to his inexperience.
The report which originally sparked Banting’s interest concerned a patient with a blocked pancreatic duct. This obstruction caused degeneration of the pancreatic acinar cells, which produce a powerful digestive enzyme. Yet it did not disable the cell clusters – known as the islets of Langerhans – which were believed to generate the hypothetical anti-diabetic agent, variously called ‘isletin’, ‘insuline’ or ‘insulin’. Banting therefore proposed tying off the pancreatic duct of an animal until its acinar cells atrophied. A purified extract from this degraded pancreas might, he thought, inhibit diabetes in a fully de-pancreatised animal.
A quiet man who disliked Banting’s abrasive manner, Collip regarded himself as answerable only to Macleod
During the summer Banting and Best accomplished this in some of their tests. Macleod was impressed enough to give them more facilities, and to offer Banting a temporary salaried position. Nevertheless, developing a reliable treatment for people with diabetes remained a formidable challenge. And after that, producing enough of the remedy for all the patients who needed it would be an equally daunting task. But Banting’s zeal remained unquenchable, and soon he was trying a new approach.
Édouard Laguesse had shown that a foetal pancreas secretes the anti-diabetic factor, but little or no digestive enzyme. Banting and Best therefore obtained foetal calf pancreas tissue from the local abattoir, ground it in a mortar, and prepared an aqueous extract which looked somewhat murky, and was obviously impure. By mid-November, injecting this into de-pancreatised animals produced outcomes that were encouraging, but still inconsistent.
Following a suggestion from Macleod, Banting and Best began using alcohol to extract the active substance. This gave a purer and more concentrated product, enabling them to get usable amounts of the agent from ordinary beef pancreas, rather than relying on scarcer foetal calf tissue. To avoid destroying the anti-diabetic factor, the alcohol had to be evaporated cautiously, and then an injectable aqueous solution prepared. This yielded better results in animal tests, but before human trials could begin, more rigorous purification was essential.
Collip, the visiting professor, was already pursuing this task. Though a year younger than Banting, Collip was an experienced biochemist with publications to his name. A quiet man who disliked Banting’s abrasive manner, he regarded himself as answerable only to Macleod (with whom he lunched regularly). The more significant Collip’s contribution became, the more Banting feared losing control of the project.
Improving the process
On 30 December 1921, Macleod chaired a meeting of the American Physiology Society at Yale University, at which Banting delivered a progress report. Banting’s results were patchy, and his presentation disorganised. Experts criticised his methods and challenged his conclusions. When he began floundering, Macleod intervened, hoping to salvage something from the wreckage. But Banting resented this rescue attempt, fearing that Macleod wanted to claim an unfair share of credit for himself. In the new year, the tensions increased further.

Injection of a human subject – Leonard Thompson – with Banting and Best’s extract began on 11 January 1922. Early results were promising, but his treatment was suspended when dangerous side-effects appeared. Meanwhile, Collip had developed a more sophisticated purification technique, involving sequential precipitation of different impurities from alcoholic solutions of increasing concentration. After the alcohol was evaporated – under a partial vacuum, since heating destroyed the ‘active principle’ – the dry product was washed with toluene (to remove fatty residues), and an aqueous solution prepared for injection.
On 23 January Thompson’s treatment was resumed with Collip’s product. This was successful, and other patients began receiving it. But as Collip tried to improve his process further, it stopped working altogether. Such unexpected setbacks are common with sensitive biochemical reactions, and in this case, pressure fluctuations in Toronto’s water supply may have affected the vacuum pump used to evaporate alcohol from his extract. Nevertheless, Banting angrily accused Collip of incompetence. Collip overcame the difficulty and continued refining his method – eventually using acetone rather than alcohol as a solvent. But he refused to reveal details to anyone except Macleod. This so infuriated Banting that only Best’s intervention stopped him punching Collip.
During the clinical trials there were further quality-control issues, but nevertheless, the results seemed miraculous – ‘it was a resurrection’, one nurse declared. Demand for the new medication became too great for any academic laboratory to satisfy. After patenting the process, the university therefore licensed the Eli Lilly Company of Indianapolis to begin mass-producing what was becoming widely known as ‘insulin’. Workers at Lilly, led by George Walden, quickly scaled up and improved Collip’s process. By December 1922 the treatment of diabetes was transformed. Surely, Stockholm would soon beckon – but to whom?
Receiving recognition
The Nobel committee’s decision to share its 1923 prize for medicine between Macleod and Banting seemed reasonable to many, for without Macleod’s support and guidance, Banting’s speculations might never have borne fruit. But Banting was incensed, believing he and Best should have shared the prize, while Macleod deserved nothing. Eventually, Banting gave half his prize money to Best, and Macleod divided his with Collip.
The appearance of insulin raised as many questions as it answered
Macleod returned to Scotland in 1928 as professor (and later dean) at the University of Aberdeen’s medical faculty, publishing useful work in physiology until shortly before his death in 1935. Banting remained belligerent – he clashed with the Hudson’s Bay Company over their treatment of Canada’s indigenous people – but did little noteworthy research before his fatal aeroplane crash in 1941. Collip died in 1965 after a distinguished career as a biochemist, having always downplayed his own role in insulin’s discovery. Best, the conciliator, asserted Banting’s prime importance in the insulin story, but still inherited Macleod’s Toronto chair. He lived until 1978.
The posthumous release of unpublished documents allowed historians – notably Michael Bliss – to retrace the pathway towards insulin. But as Bliss observed: ‘Diabetes is a far more complicated disease than anyone had realised in the 1920s. The appearance of insulin raised as many questions as it answered.’
Structural understanding
Though hailed as a miracle drug, insulin could have unpleasant side-effects – often attributed to chemical differences between human insulin and the animal-sourced injections. Naturally, the analysis – and ultimately synthesis – of human insulin became a priority. During the 1920s and 30s, several investigators confirmed that it was a protein, and identified some of its component amino acids. But its formula remained unknown, and estimates of its molecular mass varied widely.
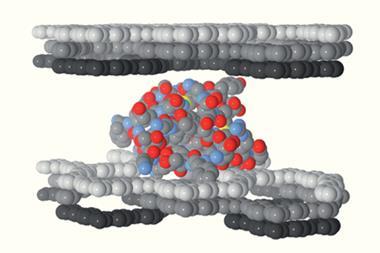
At the University of Cambridge in the 1950s, Frederick Sanger showed that the human insulin molecule contains 51 amino-acid units, in two chains linked by disulfide bridges. Its molecular mass was confirmed as 5808Da – though later work indicated that it can be stored in the body as a hexamer (with associated zinc ions). Sanger’s chromatographic analyses established insulin’s amino acid sequence, and the precise location of its disulfide bridges. But the molecule’s folded three-dimensional structure baffled x-ray crystallographers until Dorothy Hodgkin’s team at the University of Oxford solved it in 1969.
Whenever egos clash, a peacemaker like Best is always a valuable asset
Meanwhile, two research groups – led by Panayotis Katsoyanis at the University of Pittsburgh in the US and by Helmut Zahn at RWTH Aachen University in Germany – had independently accomplished the chemical synthesis of human insulin by 1965. Both routes produced low yields, and were economically unviable. Mass production of synthetic human insulin began only in the 1980s, following the application of recombinant DNA techniques by Arthur Riggs and Keiichi Itakura at the Beckman Institute in California – assisted by Herbert Boyer of the Genentec Company. Medication for diabetics is now routinely produced by adapted E. coli bacteria or yeast cells.
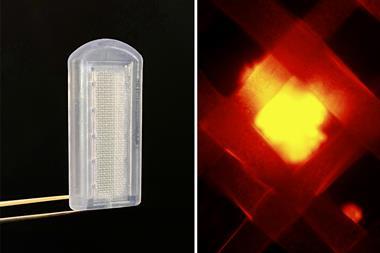
Further challenges remained. Methods for administering insulin without injections were desirable, so transplantation of islet cells began in the 1960s. (Since recipients must remain on immuno-suppressive drugs, this treatment is not recommended for general use.) In the 1970s, the first artificial pancreas was developed at Cambridge, to support vulnerable diabetics during surgery or childbirth. It was the size of a filing cabinet, but models small enough for implantation have since been developed. Orally consumable insulin is also now available, though its use is not appropriate in all circumstances.
And so the journey started in Toronto a century ago continues. One durable lesson from its story is the crucial importance of teamwork. Research groups may benefit from the inspiration of a maverick like Banting, but the finesse of experienced bench-workers like Collip is usually required to realise their vision. Oversight by a well-informed and well-connected academic like Macleod may smooth the path to success, but industrial specialists like Walden are needed to convert a laboratory triumph into a marketable product. And whenever egos clash, a peacemaker like Best is always a valuable asset.
Mike Sutton is a science historian based in Newcastle, UK







No comments yet