Multiple myeloma drug response assay could be adapted for other cancers
As part of the united effort to make healthcare technology smaller, better and cheaper, scientists in the US have developed an innovative microfluidic assay that can accurately predict how patients with a certain type of blood cancer will respond to an anticancer drug.
Cancer therapy, like the treatment of other medical conditions, often involves a degree of trial and error in the quest to find the best therapeutic option for each patient. What works for one individual will not necessarily work for another. The future of medicine lies in personalised diagnosis and treatments. Bypassing the use of often unsuccessful and sometimes potentially harmful drugs, and instead tailoring the treatment to each individual, will reduce the time and resources required to successfully treat patients.
Currently, chemosensitivity and resistance assays (CSRAs) are used to predict a patient’s response to a specific drug. However, these CSRAs are not always 100% reliable and do not take into account the influence of non-tumour cells in the overall prediction of treatment success. This is an important consideration as anticancer drugs will affect both tumour and non-tumour cells.
‘The validation of an ex vivo drug screen device for personalised medicine is a constant and tough challenge because an accurate standard just does not exist, and using patients’ clinical data for validation is an ultimate route we must go through’, explains Sihong Wang, a biomedical engineering expert at the City University of New York, US, who was not involved in the study.
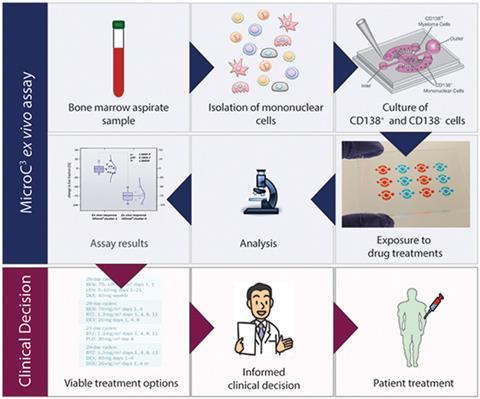
Now, Shigeki Miyamoto, from the University of Wisconsin-Madison, and colleagues have developed an assay called MicroC3 that cultures patients’ tumour and non-tumour cells together. Diffusion ports between the main well and side chambers allow molecular communication between the different cells. Furthermore, there is a size difference between the inlet and outlet ports in the device, which provide separate access to the main well and side chambers. This creates a pressure difference that facilitates passive pumping.
The MicroC3 assay predicted how patients with multiple myeloma (MM), a type of cancer affecting the plasma cells in bone marrow, would respond to the anticancer drug, bortezomib. After incubation with increasing doses of bortezomib, the MM tumour cells were stained with two different dyes to distinguish between the live and dead cells. A computer program counted the live and dead MM cells then calculated the percentage of surviving MM cells. Assay results were compared with the patients’ clinical responses to bortezomib and the results were very encouraging, with an almost 100% match.
Miyamoto’s team plan to further validate the assay with more patient samples to determine false positive and negative rates, and will be modifying the microchannel design to find out which non-tumour cell combinations give the most therapy-relevant ex vivo responses. Miyamoto will also extend the assay to other drug combinations, and he envisions that similar CSRAs could one day be developed for other cancer types too.
Wang adds that the promising results seen with the MicroC3 assay will ‘significantly encourage more researchers and bioengineers to pursue the clinical direction and help to move the field of personalised medicine forward faster, and ultimately benefit patients and society.’
References
This article is free to access until 16 July 2015. Download it here:









No comments yet