Encapsulating anticancer agents in nanoparticles can make them gentler on the rest of the body. Clare Sansom reports
Medicinal chemists working on antibiotic development have one crucial advantage over those in other therapeutic areas, perhaps particularly those in oncology: they can exploit the considerable molecular differences between bacterial and human cells and proteins. In contrast, oncologists target ordinary human cells that have been modified in various ways, picking up enough mutations to ‘go rogue’ and enter a state of uncontrolled cell division. The basic similarity between the cancer and normal cells remains, however, making it a difficult task to design a drug that is specific enough to kill tumour cells while leaving alone normal cells. Decades after the first dedicated anti-cancer drugs came on the market, and with far more drug discovery effort and resources put into cancer than into infectious disease, lack of specificity remains a key problem in cancer drug discovery.
Lack of specificity was a particular problem in the first decades of drug development in oncology. These first-generation drugs, many of which are still useful therapies for some cancers, are little more than cell poisons that target the mechanisms of cell division. This, however, also targets normal cell types that divide rapidly, including hair follicles, the cells lining the gastrointestinal tract and some types of immune cells. Cancer patients who have been prescribed this type of chemotherapy must therefore endure a characteristic pattern of side effects, including hair loss, nausea and vomiting, and vulnerability to infection. Those unfortunate enough to have been taking these drugs at the height of the Covid-10 pandemic will have been classed as clinically extremely vulnerable. Some chemotherapeutic drugs also have organ-specific toxicities, including cardiotoxicity.
In 2000, Douglas Hanahan from the Ludwig Institute for Cancer Research, Lausanne, Switzerland and Bob Weinberg from Massachusetts Institute of Technology in the US proposed a set of six ‘hallmarks of cancer’, or generic capabilities that are acquired by cells during oncogenesis; this list has subsequently been expanded to 10, all but two of which are fully validated. Mutated and dysfunctional proteins that cause a number of these, including sustaining proliferative signalling and evading cell death, are targeted by many of the more specific drugs that have been developed this century. The main problem with this type of therapeutic is knowing not only which proteins are mutated in a particular tumour but which mutations are the drivers of oncogenesis, as physiologically and histologically similar tumours often have different molecular profiles. Therefore, choice of therapy is often difficult: associating each drug with a diagnostic test (a companion diagnostic) can solve this problem, but it can also be costly and time-consuming.
In a 2021 review, Jessica Kemp and Young Jik Kwon of the University of California Irvine in the US wrote that ‘The strategy against cancer needs to shift from finding new therapies to improving existing ones… in innovative, effective, and plausible ways.’ This proposal hints at an alternative approach to that of companion diagnostics: improving the specificity, not of drug action, but of drug delivery. If a drug can be delivered to tumour cells and to those only, then even one of the old-fashioned cell poisons that targets all rapidly dividing cells can become a safe, specific drug. And one way of doing this is to hitch the drug to its own miniature chemical delivery system.
Shrunken delivery
Techniques developed over the last 20–30 years have seen drug molecules encased in or attached to precisely designed particles on the nanoscale (1–100nm) in order to deliver them specifically to the site of the tumour. These nanoparticles are designed to enhance drug permeability in a tumour, sometimes also offering a level of control of the rate of drug release and therefore of the concentration of the drug at its site of activity.
So, how can a nanoscale drug carrier target its cargo directly to a tumour, and what is there to prevent the drug from leaching out of its carrier before it arrives at its destination? The disparate mechanisms of action of nanoparticles employed to transport drugs to tumours can be divided into two basic types, known as passive and active targeting. Passive drug targeting relies on the fact that solid tumours rapidly grow their own blood vessels, in a process known as angiogenesis that is one of Hanahan and Weinberg’s hallmarks of cancer. However, these rapidly growing blood vessels are more permeable than vessels in healthy tissue, and tumours also have inefficient lymph systems. Therefore, nanoparticles carrying drugs could selectively permeate a tumour’s blood vessels and will probably end up staying there.
‘These effects, together, are known as the enhanced permeability and retention effect and it is thought that this could provide a starting point for selective nanoparticle delivery in the absence of a specific target on tumour cells, although there is scepticism about its utility,’ explains Kwon. In contrast, actively targeted nanoparticles have components that are designed to bind to specific proteins that are expressed by and embedded in the membranes of tumour cells, but even here, the drug must first reach the cancer cell in order to bind to the target protein.
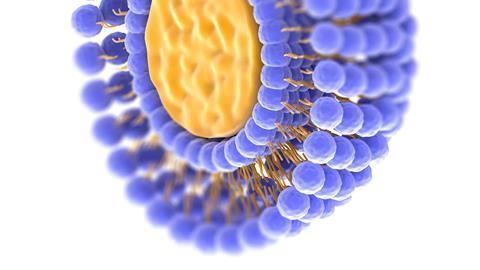
The modern oncologist’s armoury of nanodrugs may be varied, but the short history of nanomedicine has been dominated by one type of particle: liposomes, the first nanoparticles to be successfully employed in drug delivery. In simple terms, these are spherical vesicles formed from lipid bilayers, with the drug molecules encapsulated in the internal aqueous phase of the liposome. Most are relatively large on the nanoscale, with a diameter close to 100nm.

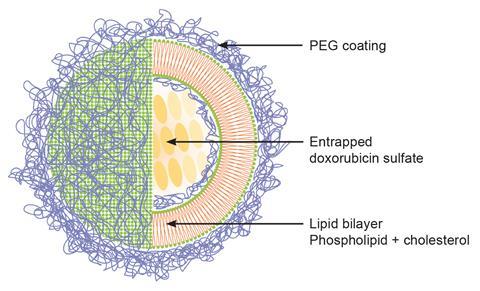
The first of these ‘nano-drugs’ to be approved by the US Food and Drug Administration was Doxil, in which the commonly used chemotherapy drug doxorubicin is encapsulated in a PEGylated nano-liposome. This drug – a topoisomerase inhibitor with a planar aromatic core that intercalates between base pairs in the DNA double helix, and which targets rapidly-dividing cells – was licensed in 1974 and is still a first-line treatment today. Doxil was developed and patented in a collaboration between Chezy Barenholz of the Hebrew University of Jerusalem in Israel, Alberto Gabizon (now an oncologist at Shari Zedek Hospital in Jerusalem) and a small pharma company, Liposome Technology in California, US. ‘I was already studying liposome biophysics and biochemistry when, in 1979, I was approached by the head of oncology at Hadassah University Hospital in Jerusalem,’ remembers Barenholz. ‘He was looking for a project for a young oncologist who wanted to spend a couple of days a week working on cancer research.’ The oncologist concerned was Gabizon; he and Barenholz chose to explore whether liposomes could improve the specificity and targeting of drugs for hepatocellular carcinoma. This intractable type of liver cancer is particularly common in East Asia and Japan. Doxorubicin was chosen as the ‘cargo’ of the delivery system because of its efficacy, and because it can be made to fluoresce and so be easily traced in the body.
Enhancing efficiency
By the time the group had developed a liposomal preparation of doxorubicin and shown it to work in mouse models, they already had Liposome Technology (LTI) lined up to support the development of liposomal doxorubicin. First-in-man trials, however, were disappointing: the drug was rapidly released by the liposomes so its concentration at the tumour site was too low to be effective. This led the collaborators to try to develop a better liposomal doxorubicin formulation. Barenholz and his student Gilad Haran (now at the Weizmann Institute) developed nano-liposomes that stably encapsulated doxorubicin at high enough concentration to treat humans. This invention was licensed to LTI in 1988, which patented the use of PEGylated liposomes for drug delivery. These are long-circulating nano-liposomes are coated with moieties of polyethylene glycol (PEG). ‘PEG is a saturated polymer with no double bonds, so its molecules are extremely flexible,’ says Barenholz. ‘Due to its high oxygen content it binds many water molecules, making a bulky coating that can protect the surface of the liposome from serum protein binding. It also inhibits Doxil’s interaction with blood cells, including cells of the immune system, so the liposomes reach the tumour intact and loaded with their payload.’ As Doxil liposomes bind serum proteins much less readily than the non-PEGylated nano-liposomes they are less visible to the human immune system and have been termed stealth liposomes.
Doxil was approved by the FDA in 1995 and the European Medicines Agency in 1996 and since then it has been sold globally. Its patents expired in 2009–2011 and there are now four generic versions including one from Ayana Pharma, a company founded by Barenholz. Doxil and its generics are significantly less cardiotoxic than non-encapsulated doxorubicin, and they have been used successfully to treat over a million cancer patients worldwide. Furthermore, Barenholz explains that the exact mechanism through which the drug is selectively released within the tumour ‘remained a mystery’ until as late as 2015. Then he and a student, Liza Silverman, discovered that ammonium ions and ammonia produced selectively in tumours may be responsible for doxorubicin’s release from the nano-liposomes in the tumour tissue.
Today, Doxil is prescribed most often for advanced ovarian cancer and for Kaposi’s sarcoma, a form of skin cancer that gained notoriety at the start of the HIV/Aids epidemic as a frequent early sign of infection. And liposomal (most often stealth liposomal) preparations of many other cancer drugs are in active development: more than a thousand clinical trials of such preparations are currently listed on the ClinicalTrials.gov database.
An inorganic option
The features of solid tumours that make passive targeting by nanoparticles possible – the distinct tumour body, the leaky vasculature and the inefficient lymphatic system – are not found in leukaemias, lymphomas and other blood cancers where tumour cells circulate in the blood and lymph systems. Coupling PEG and ligands onto nanosystems that enhance their circulation time and help evade the immune system can be just as effective for these cancers, and these methods generally use active targeting.
‘Standard chemotherapy drugs can be incorporated into nanoparticle carriers that are designed to bind specifically to proteins expressed on the surfaces of blood cancer cells,’ explains Tamer Elbayoumi of Midwestern University in the US state of Arizona. Indeed, these targeted carriers are often liposomes with antibodies or other protein ligands that bind to these tumour markers embedded on their surfaces as well as, or instead of, polyethylene glycol. The cancer cell surface proteins targeted are often cell surface antigens known as clusters of differentiation – CD19, CD20 and the like – or receptors for proteins involved in DNA replication, such as dihydrofolate reductase. ‘It is essential to pick a target protein that is overexpressed on the surface of each patient’s tumour cells,’ adds Elbayoumi. ‘Some of the potential targets are quite generic, but others require a precise differential diagnosis.’
Gold is the commonest noble metal used in nanomedicine
Nanoparticles used in drug delivery and elsewhere in medicine may be inorganic as well as organic. Tiny particles of pure solid elements, and particularly of the noble metals, have many medical uses including in cancer drug delivery. This term is used to describe a rather loosely defined category of transition metals. They are so named not from their beauty or historic uses (although the category includes all precious metals except silver) but from their inactivity, particularly resistance to corrosion and oxidation. These properties make them ideal for medical applications, a fact that has been known for many generations, perhaps since teeth were first filled with gold.
Gold is the commonest, although not the only, noble metal used in nanomedicine. A suspension of nanoscale particles of pure gold, known as ‘colloidal gold’, will preferentially bind to tumours and while this has no curative effect on its own it can potentiate other therapies, particularly heat therapy or hyperthermia. This was discovered through the clinical observation that fever could sometimes, paradoxically, be good for cancer patients. Holding a tumour at, say, 42–45°C will not only kill cancer cells directly but potentiate the effect of radiotherapy; holding a patient’s body at this temperature, however, would be fatal. The great difficulty with using heat as a therapy has been one of directing that heat precisely enough to cause heat stress in the tumour only. This has now been achieved by a nanoscale method. First, colloidal gold particles are delivered to bind to the tumour, and then it and its surrounding tissue are irradiated with a light or near infra-red (NIR) laser. The gold particles convert this radiation into heat energy, thus heating the tumour but not the surrounding tissue to a high enough temperature to cause toxic heat stress.
Most nanomedicines are still costly and difficult to manufacture, and particularly difficult to manufacture consistently. Tiny, subtle differences in the manufacturing process can have significant effects on particles’ activity, as John Hertig from Butler University in Indianapolis, US, explains: ‘Manufacturing defines the particle, and the particle defines the medicine.’ And manufacturing processes are harder to control in drugs that are off patent, as Doxil has been for over a decade. Quality control is harder with these ‘nanosimilars’ than with the original patented formulation. Nanosimilars are badly needed if these important drugs are to be made readily available to cancer patients worldwide, but the manufacturing processes, and therefore the resulting drugs, must be precise, accurate and trustworthy.
Rapid developments in a completely different branch of medicine might offer a way forward, however. After all, the carriers for the transformational Pfizer and Moderna mRNA Covid vaccines are lipid nanoparticles. These resemble liposomes but differ in their lipid composition and also in that they have a lipidic core rather than a water core, with the nucleic acid encapsulated in that core. ‘The companies that brought us the Covid vaccines are now working on mRNA vaccines for many other diseases, including cancer vaccines,’ says Kwon. And the recent success of the new South African mRNA vaccine hub in developing ‘reverse engineered’ generic vaccines suggests that hurdles preventing the production of precisely engineered generic nanodrugs should be surmountable.
Clare Sansom is a science writer based in Cambridge, UK











No comments yet