

Two billion-dollar acquisitions in late December 2023 confirmed renewed interest in radiopharmaceuticals from big pharma companies. The deals highlight the potential for growth in this class of targeted cancer therapeutics.
On 26 December, Bristol Myers Squibb agreed to buy RayzeBio for $4.1 billion (£3.2 billion), and a day later Eli Lilly completed its $1.4 billion acquisition of Point Biopharma. RayzeBio has two potential cancer therapies based on actinium-225 in clinical trials, while Point has a pair of lutetium-177 therapies in phase 3 trials.
Radiopharmaceuticals have been around for decades. The basic aim is to stick a radioisotope onto a tumour so that it can release energy and kill the cancer cells. For example, radioactive iodine collects in thyroid cells, so has been used against thyroid cancer. While a radium-233 treatment (Bayer and Algeta’s Xofigo) targets bone cells because of its similarity to calcium and is used for patients whose prostate cancer has metastasised to their bones.
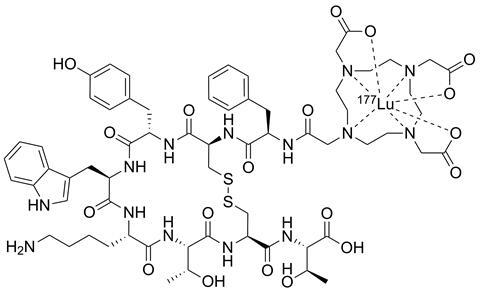
More sophisticated designs involve a cancer targeting molecule, a linker and a chelating agent to hold the radionuclide in place. The field reached a commercial tipping point in 2018 when the US Food and Drug Administration (FDA) approved Lutathera (lutetium-177 oxodotreotide) from Novartis for neuroendocrine tumours.
Then, in May 2022, the agency approved a second Lu-177 therapy from Novartis – Pluvicto (lutetium-177 vipivotide tetraxetan) – for metastatic prostate cancer, a late-stage cancer with a 5-year survival rate of less than 30%. ‘These patients are basically out of options. The results were stunning, with a 60% reduction in the risk of disease progression, 40% reduction in risk of death,’ says Andy Hsieh, a biotech analyst with William Blair, an equity research firm.
Further positive results from Novartis followed. ‘That really put radiopharmaceuticals on the map, and it catalysed a lot of investor enthusiasm,’ says Hsieh. Prostate is the most common cancer in men and Pluvicto closed in on blockbuster status in 2023 with sales of $980 million.
Investors and larger firms are now tracking pipelines in the field, from a host of companies such as Mariana Oncology, Fusion Therapeutics, Alpha9 Theranostics and Artbio. ‘There is a resurgence of interest and big pharma is not sitting around. They’re all looking at radiopharmaceuticals very closely,’ says Hsieh.
‘What we’re experiencing now is a renaissance,’ says Germo Gericke, chief medical officer at Ariceum Therapeutics, a private company headquartered in Germany with a pipeline of novel radiopharmaceuticals for imaging and treating cancer.
‘This field has been around for a while, but people are realising that it has a lot to offer patients, especially those with advanced disease or few other treatment choices,’ says David Mankoff, a radiologist and nuclear medicine physician at the University of Pennsylvania, US.
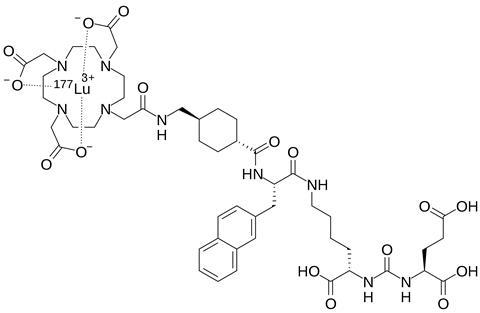
Both Pluvicto and Luthatera carry 177Lu, which is a medium energy beta-emitter. It also emits photons that can be used for imaging. Point Biopharma has another 177Lu agent in phase 3 clinical trials for prostate cancer.
Other beta emitters are being investigated. Australia’s Clarity Pharmaceuticals combines its targeting molecules with copper-64 and copper-67 for diagnosis and therapy, respectively. Its pipeline includes candidates in clinical trials for prostate cancer and breast cancer, as well as for neuroblastoma. Getting hold of 67Cu was once difficult, but commercial supplies are coming online.
Enter the alpha-emitters
Several of the therapies in development carry alpha-emitting nuclides, rather than beta emitters. While beta emission can penetrate and destroy cells over a distance of few millimetres, alpha emitters can send out more energy, over a more localised range of nanometres, making them more destructive and precise in killing just a few nearby cells.
‘You get more bang for your buck, so much more energy into the tumour per anchor point,’ says Gericke. ‘If beta emission is like a rifle shot, alpha emission is like a major cannon on a warship.’ The cancer cells suffer more damage and more double-strand DNA breaks, which are more difficult for the cells to repair than single-strand breaks.
Fusion Pharma is one of the companies pursuing actinium-225, a popular alpha-emitter moving toward the market, but not yet approved. Fusion announced a phase 2 trial for patients with progressing metastatic prostate cancer, and who had already received a beta-emitting therapy such as Pluvicto.
RayzeBio’s lead candidate, RYZ101, also employs 225Ac. The firm began enrolling patients with gastroenteropancreatic neuroendocrine tumours expressing somatostatin receptor 2 (SSTR2) for a phase 3 trial last year.
‘The allure of using alpha emitters, specifically actinium-225, is driving the interest of big pharma,’ says Hsieh. He describes investment activities in radiopharmaceuticals as spectacular, with companies attracting close to a hundred million dollars in early-stage Series A funding, and hundreds of millions in Series B funding to support firms’ growth and scale-up. Mariana Oncology alone garnered $175 million in Series B financing last September.
‘There’s quite a range of other alpha emitting isotopes that are attracting high interest and we’re trying to understand how best to deliver those because the chemistry is complicated,’ says Steve Archibald, a radiochemist at King’s College London, UK. The initial alpha emission can initiate a chain of further alpha-emissions, with Ac-225 for example undergoing four alpha decays (and two beta decays) to produce stable bismuth-209. This can be useful in terms of maximising damage to tumour cell, but could potentially also lead to off-target damage if daughter nuclides end up circulating round the body.
If beta emission is like a rifle shot, alpha emission is like a major cannon on a warship
An isotope of the rare element astatine, At-211, is also an alpha emitter; a recent review noted it was in clinical trials in the US and Japan. Mankoff points to preclinical research for neuroblastoma with At-211 from another group at the University of Pennsylvania and hopes to move an At-211 agent towards the clinic himself for adult and childhood cancer.
More popular is lead-212, with multiple firms moving this into radiopharmaceuticals. ‘There is an interest in 212Pb as an alpha-emitter, differentiating it from actinium, in that it has no daughter nuclides, lowering the risk of freely circulating radioactive nuclides,’ explains Gericke. Lead-212 undergoes beta-decay with a convenient 10.6h half-life to produce 212Bi, which then rapidly decays to 208Pb by a combination of alpha and beta emission.
The firm Artbio describes 212Pb as clinically ideal because it is short lived, has high stability and can be imaged in the body. Its pipeline focuses on 212Pb for prostate cancer and solid tumours.
Meanwhile, in 2023, Orano Med began a clinical trial of a 212Pb targeted therapy for neuroendocrine cancers. The company’s mostly preclinical pipeline with 212Pb aims to target different cancer receptors or antigens for breast and prostate cancer, as well as lung cancer. In January, Lantheus signed a strategic agreement with Perspective Therapeutics, buying a 20% stake in the firm for $33 million, to push forward therapy based on 212Pb for neuroendocrine and prostate cancers.
Supplies strained
Therapeutic radiopharmaceuticals generally have half-lives of hours to weeks, so stockpiling is not possible, requiring constant supply. ‘There are not that many production sites globally,’ says Archibald, of radioisotopes generally. A UK government report in 2017 noted that six fission reactors generate more than 90% of medical isotopes worldwide.
Actinium-225 supply is certainly an issue when it comes to prospective therapies. ‘Global production of 225Ac is only sufficient for treatment of a few hundred patients per year. This makes it difficult and very costly to access,’ says Erik Arstad, radiochemist at University College London, UK. ‘Most appealing alpha-emitters are not sufficiently available to allow scale-up for routine clinical use. It’s a massive bottleneck.’
But production is advancing. ‘There are lots of government initiatives and also private enterprise investments looking at medically relevant radioisotopes,’ says Hsieh. In the UK, a project called Arthur – advanced radioisotope technology for health utility reactor – has been proposed by the Welsh government.
The US Department of Energy Isotope Program (DOE IP) named 225Ac as a critical medical isotope and has invested in new production methods. For now, it mainly originates from decay of thorium-229 leftover from nuclear programmes in the mid-20th century. Each month, scientists at Oak Ridge National Laboratory separate out 225Ac from the other nuclides that decay from thorium. DOE IP has been advancing accelerator-produced 225Ac.
There are private efforts too. Fusion Therapeutics partnered with a subsidiary of nuclear technology provider BWX Technologies in January, to produce 225Ac at its manufacturing plant and a commercial cyclotron facility in Canada.
Global production of 225Ac is only sufficient for treatment of a few hundred patients per year
In the UK, a spinout company from the University of Bristol called Astral Systems has developed a compact fusion reactor to create medical isotopes. ‘With the expected increasing clinical impact, we need to have more supply infrastructure for radionuclides,’ says Archibald, who has worked with Astral.
Lead-212 production, meanwhile, is being pursued by multiple companies. Orano laid the foundation stone for a facility dedicated to producing 212Pb-based radioligand therapies in northern France in February, Europe’s first such industrial-scale facility. Meanwhile, Point Biopharma has a facility licensed for alpha and beta-emitting nuclides in Indianapolis, US. Industry watchers believe that this site was a major attraction for neighbour Eli Lilly’s recent purchase of Point.
Companies can face production challenges, aside from the radionuclides. In May 2022, Novartis suspended production of Lutathera and Pluvicto at plants in Italy and the US to address potential quality issues in its manufacturing process, which impacted supply.
Early this year, Novartis received approval for a large plant in Indianapolis, purpose-built for radioligand therapy. ‘We are not talking about regular drug manufacturing facilities. You need specialised facilities to produce radiopharmaceuticals and to be constantly churning out doses,’ says Archibald.
Investors and companies see opportunities in these supply issues. There has been a lot of emphasis on isotope production and Good Manufacturing Practice-compliant manufacturing capacity, confirms Gericke. He predicts that capacity for radiopharmaceuticals will grow steadily, akin to monoclonal antibodies over the last 15 years. ‘I guess that over the next 12–18 months, radioligand contract manufacturing will become – not a commodity per se – but an available service,’ he adds.
Hsieh is optimistic around manufacturing and logistical teething problems. ‘It is analogous to cell therapy, where there was a lot of investment in building up the manufacturing and supply chain,’ he says. ‘Its success really lends confidence in the radiopharmaceuticals space.’ Like cell therapy, the clock is running in terms of getting a radiopharmaceutical to its patient.
New targets
As well as the radionuclide payload, companies are aiming to expand the range of proteins or receptors that can be targeted, beyond prostate-specific membrane antigen (PSMA) and SSTR2. ‘Ideally you want [to bind to something] that is almost exclusively expressed on the tumour and not healthy tissue,’ says Gericke. That could be achieved using small molecules or peptides – as seen in Lutathera and Pluvicto – or with biomolecules like antibodies or antibody fragments. ‘Opinion is divided around [which] will be more successful,’ says Gericke. He describes himself as a big fan of small molecules, partially due to their lower bone marrow toxicity.
You can overcome biological resistance by using very potent physical energy to destroy the cancer selectively
For example, Ariceum has applied to UK regulators to begin a trial of an iodine-123 labelled small-molecule inhibitor of DNA-repairing enzyme poly(ADP-ribose) polymerase (PARP), in patients with glioblastoma, an aggressive type of brain cancer. And the lead candidate at Mariana Oncology is a peptide engineered to carry actinium-225 and hit small-cell lung cancer, an aggressive and difficult-to-treat cancer.
Meanwhile, Belgian biotech Precirix uses small antibodies from camelids to target cancer; its lead candidate uses a single-domain antibody linked to beta-emitting iodine-131 to target metastatic HER2-positive breast cancer.
A big cancer market awaits. ‘Cancers that are difficult to cure are particularly appealing for targeted radiotherapy,’ says Arstad. Mankoff agrees that it can be an effective approach to treat other refractory cancers like ovarian and lung. ‘You can overcome biological resistance by using very potent physical energy in the form of these radioisotopes to destroy the cancer selectively,’ he adds.
‘Previously, profitability was not seen to be there with radioisotope diagnostics,’ says Archibald. ‘But now the combination of the therapeutic and diagnostic has seen large pharma shift its attitude.’













No comments yet